





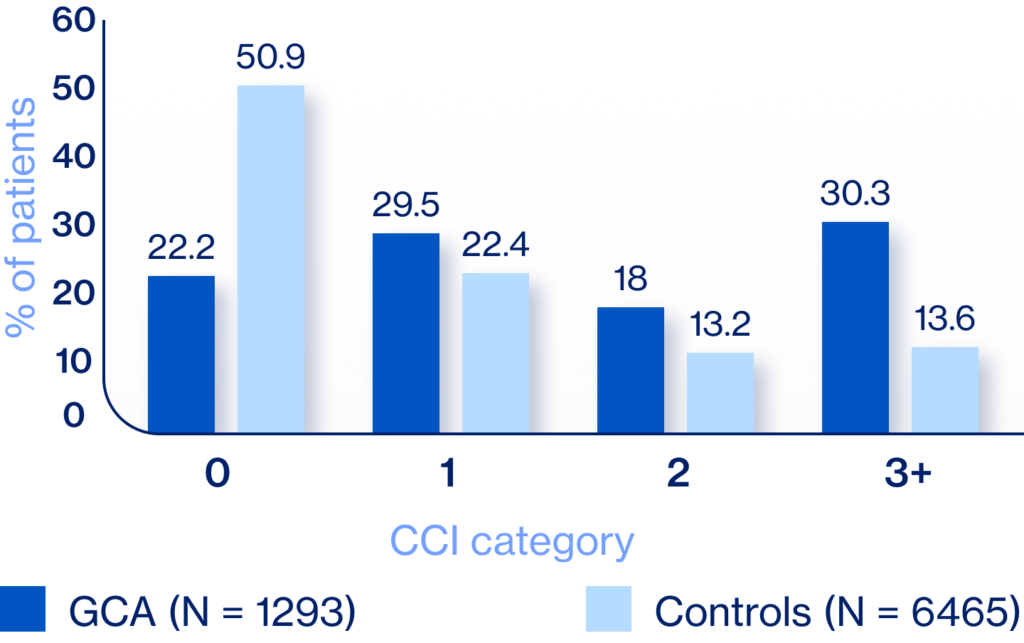
Differentiating between GCA and aches/pains from comorbid conditions5
Understanding risk of AEs with prolonged corticosteroid use1-4

Explaining rationale and importance of corticosteroid tapering to balance benefit vs AEs5,6

Incorporating physical therapy to address comorbid pain7 and reduce corticosteroid dependence



ACR guidelines recommend6:
“For patients with newly diagnosed GCA, we conditionally recommend the use of oral corticosteroids with IL-6 inhibitor over oral corticosteroids alone”


GCA relapse: reappearance of ≥1 GCA symptoms11
ACR guidelines recommend6:
“For patients with GCA who experience disease relapse with symptoms of cranial ischemia, we conditionally recommend adding a noncorticosteroid immunosuppressive agent and
increasing the dose of corticosteroids over increasing the dose of corticosteroids alone”



Large vessel
involvement
present in up to 83% of patients with GCA;13-15 can occur with or without cranial GCA13

Aortic aneurysm risk
increased 17-fold for patients with GCA vs age/sex matched comparators16

Risk of death
increased 3.4-fold for patients with aortic aneurysm vs those without large vessel involvement17

ACR guidelines recommend6:
“For patients with suspected GCA and a negative temporal artery biopsy result (or results), we conditionally recommend noninvasive vascular imaging of the large vessels with clinical assessment to aid in diagnosis over clinical assessment alone”

