- Dr. Mease and Dr. Khattri • August 2023

Philip Mease, MD
Director of Rheumatology Research, Swedish Medical Center Providence St. Joseph; and Clinical Professor, University of Washington School of Medicine

Saakshi Khattri, MD
Rheumatologist and Dermatologist, Icahn School of Medicine at Mount Sinai







At Week 16, subjects classified as nonresponders (defined as not achieving at least a 20% improvement in either or both TJC and SJC at both Week 12 and Week 16 compared to baseline) had the option to add or modify rescue concomitant medications/therapy.

The overall safety profile of RZB observed in subjects with PsA treated with RZB is generally consistent with the safety profile in subjects with plaque psoriasis, with the addition of hepatic events — for example, increased ALT and AST, but no serious hepatic events reported — and hypersensitivity reactions.

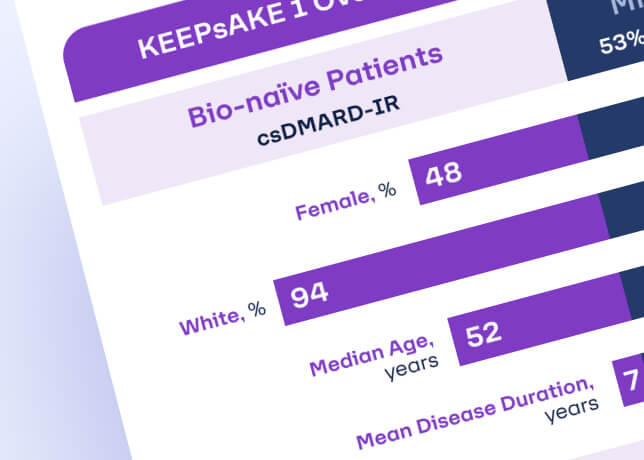
Find out more about composite measures in bio-naïve patients with PsA treated with RZB

How important are treatment targets in your assessment of patients with PsA?
How likely are you to use a composite measure like the MDA in monitoring a patient with PsA?
How likely are you to consider a selective IL-23 p19 inhibitor if a bio-naïve patient with PsA is not meeting treatment targets?