- Dr. Curtis & Dr. Winthrop • October 2025
Jeffrey R. Curtis, MD, MS, MPH
Professor of Medicine, Epidemiology, and Computer Science
Division of Clinical Immunology and Rheumatology
University of Alabama at Birmingham
Kevin Winthrop, MD, MPH
Professor
School of Medicine,
Divisions of Infectious
Diseases and Ophthalmology
School of Public Health
Oregon Health and Sciences University

Consider your patient’s understanding and context,
and meet them where they’re at

Highlight medication risk
by sharing important safety content

Anchor to your patient's baseline risk
for outcomes related to the disease itself and other risk factors (e.g. comorbidities)

Tune in to your patient's motivation and emotions,
and commit to continued discussions

Treatment goals for RA: Is it time to transition MOAs?
Rheumatologists Dr. Christina Charles-Schoeman and Dr. Manish Jain discuss their approaches to setting and pursuing treatment goals for patients with poorly controlled RA after TNFis

RA Risk Radar: Heart Disease, Infection, and Malignancy
Rheumatologists Dr. Jeffrey Curtis and Dr. Jon Giles discuss the risk of comorbidities that can occur as a consequence of uncontrolled inflammation in RA
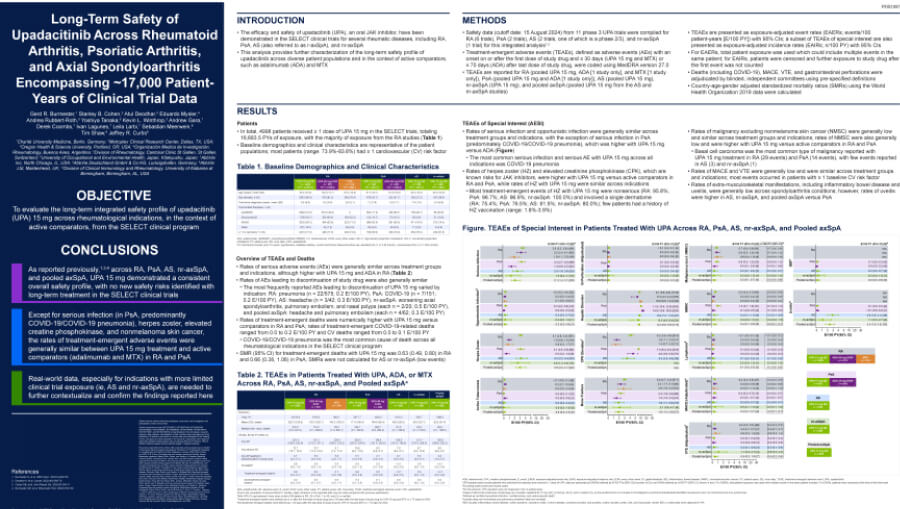
Long-term safety of a JAKi across ~17,000 patient-years
Presented at EULAR 2025, this poster examines the long-term safety of UPA across multiple Phase 3 trials


